
Plantar Fasciitis also known as Plantar heel pain (PHP) or Plantar fasciopathy is a common condition that affects the heel in over 2 million people each year. It is estimated that almost 10% of the general population is affect by PHP at some point in their lives.
The terminology is also a point of contention with the suffix “-itis” often incorrectly indicating that there is an inflammatory process underlying which histological studies of the plantar fascia reveal is not the case. There can be inflammation of surrounding soft tissues etc but not of the plantar fascia itself.
Anatomy and Function
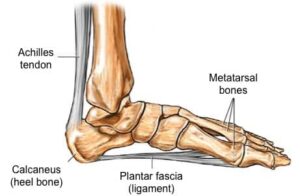
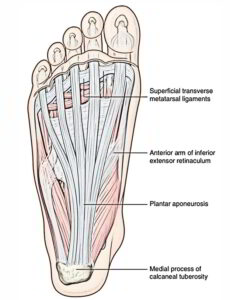
The plantar fascia or plantar aponeurosis is a fan shaped connective tissue attaching onto the calcanea tubercle and fanning to attach onto the more distal aspect of the plantar metatarsal heads. There is a medial, central and lateral band. It is composed of Type 1 collagen fibres which is also what tissues like the Achilles and patella tendons are made of. The plantar fascia serves as an elastic storage of energy during the gait cycle storing energy during the transition from heel strike to toe off during walking/running, in particular the extension of the big toe and lesser toes leads to the “Windlass effect” which can be likened to a series of pulleys which engage the medial band of the plantar fascia and central/lateral bands respectively.
Symptoms
There are several hallmark symptoms that feature in most cases such as a throbbing medial plantar heel or pain after the first steps after a period of inactivity or rest. Palpating the medial aspect of the plantar calcaneus generally produces a sharp stabbing pain. It is imperative that an accurate diagnosis is obtained, as the management for other pathologies can be quite different.
Differential diagnosis
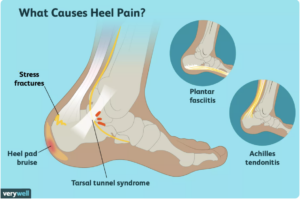
Generally a thorough clinical history and examination will elicit a satisfactory clinical diagnosis, however, imaging modalities such as ultrasound and MRI will rule out other causes of heel pain. Some other pathologies that can present quite similarly include:
-Fat pad bruising
-Bursitis
-Baxter’s Neuritis or Neuroma
-Calcaneal Stress fracture
-Muscle strain
-Insertional Achilles tendinopathy (more posterior located pain)
A sonographic image of PHP will typically show thickening of the plantar fascia at the insertion (>3mm thickness is clinically significant) or minor or partial tearing. Although the presence of significant tears will often be accompanied by a traumatic event or memory of a particularly sharp, painful sensation during movement.

Risk Factors
We know this condition to be particularly prevalent in those with high BMI, taller or in occupations with long periods of standing. It can often be brought about where there is a high spike in training loads or “too much too soon” as far as exercise or physical activity. This can precipitate due to lack of time allowing for adaptation of the connective tissues. Inactivity can also be a factor, with occupations where there are lengthy periods of sitting, which leads to shortening and tightening of hamstrings and calves which can affect the plantar fascia function.
Calf tightness and poor ankle mobility are often factors in PHP, due to the Achilles tendon and plantar fascia sharing fascial attachments and a common anchor point in the calcaneus.
Footwear can be an important consideration, where tight toe boxes, high heels and poor cushioning can negatively impact the function of the feet and lead to development of foot pathologies.
Management

In the initial term use of rigid taping to perform a low dye strapping is highly useful to unload the painful plantar fascia and provide support for the medial arch during ambulation. This can be continued up to 2-3 weeks on initial management. This also forms a good test to evaluate whether the use of orthoses will provide pain relief and improvement of biomechanics.
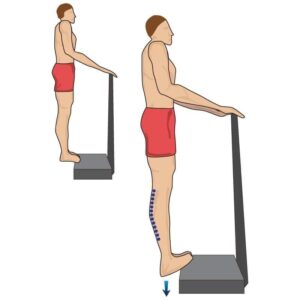
Often, we have to address the proximal factors such as excessive calf tension that is restricting the ankle and puling tension through the plantar fascia. A dedicated calf stretching and strengthening regime should effectively lengthen the calf muscle whilst improving strength in the plantarflexors at the ankle and muscles of the foot.
Careful examination of the patient’s gait cycle and biomechanics may reveal some clues that may contribute to the pathology. We may look to optimise this in the form of orthotic therapy and footwear prescription. It may be the case that certain footwear is exacerbating the issue or is providing poor off-loading or cushioning of the painful insertion point of the plantar fascia. This is where we could look to improve cushioning with appropriate footwear options or orthotic accommodations.
Manual Therapies and Other Interventions
In the case of recalcitrant cases of PHP, we may look at further interventions such as Extracorporeal Shockwave Therapy, Plasma Rich Platelet injection or Corticosteroid injection.
There is poor evidence for good long term outcomes with CSIs and PRP, however some promising results have emerged looking at ESWT in treatment of PHP. Often times, combinatorial therapies such as Stretching/Strengthening of calf muscles and ESWT have had great synergistic effects. The bottomline being to address the factors that are contributing, as PHP is often of a multifactorial cause.
Dry needling and soft tissue therapy, despite poor evidence in the literature, can have benefit as far as pain relief and improvement of symptoms or excessive muscle tension, and can be a useful adjunctive therapy.
